Session Information
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Data about heart failure (HF) in patients with psoriatic disease (PsD) are sparse. The aims of the study were to: 1) determine the incidence and predictors for HF in patients with PsD and 2) describe their electrocardiographic (ECG) and echocardiographic (TTE) findings.
Methods: A cohort analysis was conducted on patients followed prospectively from 1978 to 2018 in the psoriatic disease program. Participants were assessed according to a standard protocol that included demographics, medications, measures of disease activity and comorbidities. The primary outcome was the first incident event of HF. HF events were further classified into ischemic and non-ischemic HF. Potential HF events were identified by searching the cohort database and linkage with provincial hospitalization and mortality databases. Patients with HF prior to study entry were excluded. The association between cardiovascular risk factors, measures of disease activity and occurrence of HF events was assessed using Cox proportional hazard models with time varying co-variates. Review of medical records identified ECG and TTE findings in patients with HF.
Results: A total of 1994 patients with PsD with 22,437 patient years were analyzed. During the follow-up period, 64 new HF events occurred (38 ischemic, 26 non-ischemic). The cumulative prevalence of HF by the age of 70 and 80 years was 1.4% and 3.7%, respectively. The incidence rate of first HF event during the study period was 2.85 per 1000 patient years. Of the 41 cases with available medical records, there were 19 cases of ischemic HF and 22 cases of non-ischemic HF (arrhythmias, cardiomyopathy and valvular dysfunction). In all events, the most common ECG findings were atrial fibrillation (22%), bundle branch blocks (29%) and pathological Q waves (33%). In all HF events, TTE revealed 37% reduced ejection fraction, 29% preserved ejection fraction, wall motion abnormalities (61%), left ventricular hypertrophy (41%) and valvular abnormalities (32%).
On multivariate analysis (Table 1), the following variables were independent predictors for all HF events: ischemic heart disease (p< 0.001), adjusted mean (AM)-tender joint count (TJC), AM-swollen joint count, AM-ESR, and HAQ (all p< 0.05). The strength of association of disease activity measures was higher when the analysis was restricted to non-ischemic HF as the outcome, with pain score, AM-TJC, AM-SJC, ESR and damaged joint count as independent predictors (all p< 0.05). The strongest predictor of ischemic HF was prior ischemic heart disease and additional independent predictors included: AM-ESR and HAQ (p< 0.05). Being in a minimal disease activity state was protective for all HF and ischemic HF (p< 0.05).
Conclusion: Increased risk of HF in PsD is associated with a combination of traditional cardiovascular risk factors and disease activity, particularly in patients with non-ischemic HF. The effect of inflammation on HF may be partially independent of atherosclerotic disease.
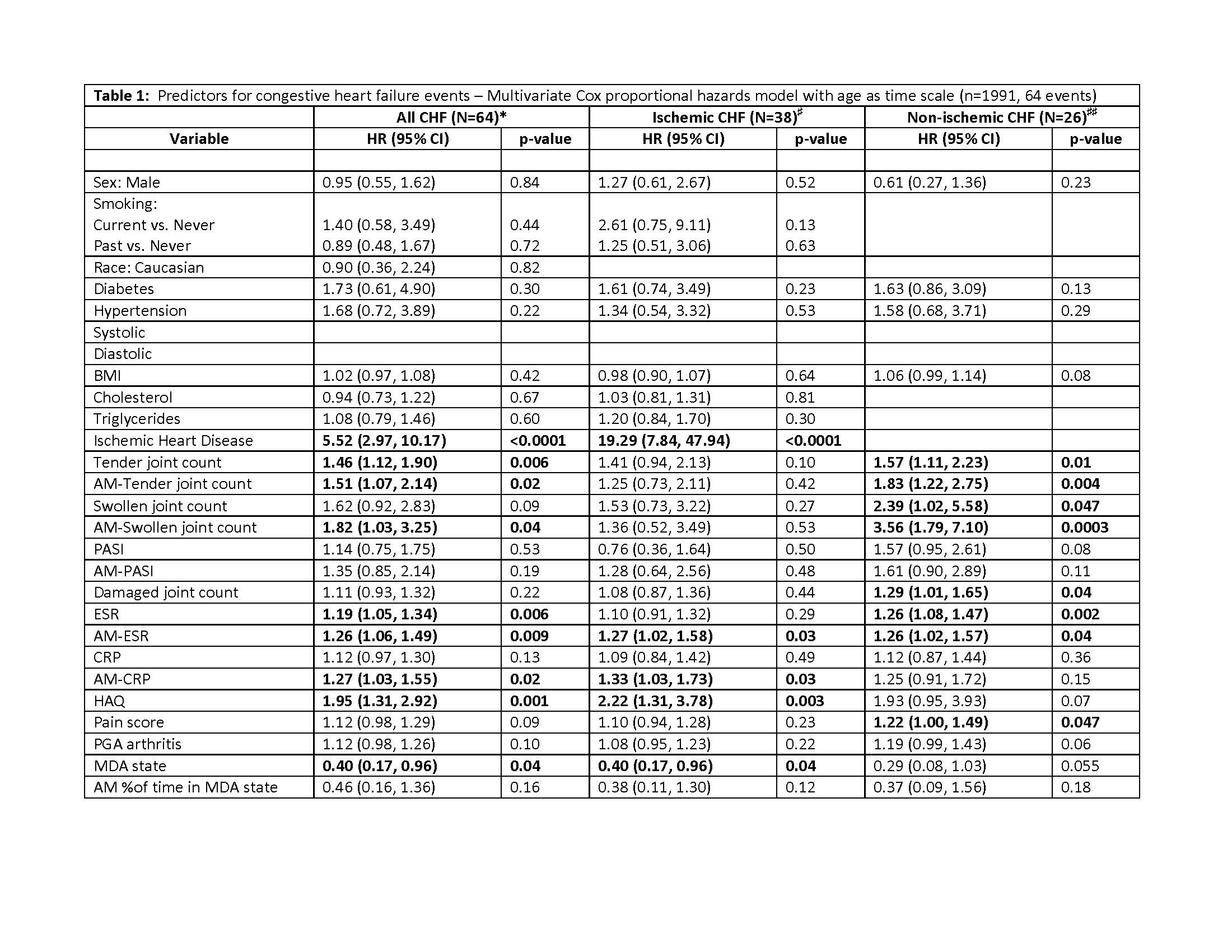
Table 1
To cite this abstract in AMA style:
Koppikar S, Colaco K, Harvey P, Chandran V, Gladman D, Cook R, Eder L. Incidence and Predictors of Heart Failure in Patients with Psoriatic Disease – a Cohort Study [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/incidence-and-predictors-of-heart-failure-in-patients-with-psoriatic-disease-a-cohort-study/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incidence-and-predictors-of-heart-failure-in-patients-with-psoriatic-disease-a-cohort-study/