Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Accelerated atherosclerosis remains the major cause of late death (after 5 years) in systemic lupus erythematosus (SLE). Yet, the “traditional” cardiovascular risk equations (such as Framingham) consistently underestimate the risk. We revised our data-driven formula for cardiovascular risk in SLE, to base it on data collected during just the first year of follow up in a longitudinal cohort, versus two years.
Methods: We included 1,721 patients from a longitudinal cohort. They were assessed for cardiovascular adverse events (stroke, myocardial infarction [MI], angina or coronary procedures, claudication, or congestive heart failure), for traditional cardiovascular risk factors (age, sex, ethnicity, systolic blood pressure, total cholesterol, smoking, and diabetes mellitus) and for SLE-related risk factors (low C3 and C4, anti-dsDNA, proteinuria, SELENA SLEDAI score, and history of lupus anticoagulant and anticardiolipin) during the first year of follow up. Using Cox proportional hazards modeling, SLE formulas to calculate the 10-year risk of a subsequent cardiovascular event were derived and compared to the Framingham (for all outcomes) and to the American Heart Association/American College of Cardiology (AHA/ACC) formula (for MI and stroke).
Results: Of the 1,721 patients, 168 had a cardiovascular event after the first year of cohort participation, and during cohort participation. Of these 168 events there were 70 strokes, 27 myocardial infarctions, 27 patients with angina or requiring coronary procedures, 14 patients with heart failure, 13 with peripheral artery disease, 11 with claudication, and 6 with more than one type of event. Table 1 shows the hazard ratios for rates of a cardiovascular event. Using the hazard ratios from Table 1, we compared the estimated 10-year risk based on our formula with the calculated risk using the Framingham formula (Table 2). We also derived a formula for a more restricted definition of cardiovascular event (cardiovascular death, MI and stroke) using hazard ratios from a separate Cox proportional hazards model and derived a formula that was compared with the AHA/ACC formula (Table 3). Using our formulas, which includes SLE-related risk factors, the risk was substantially higher than the estimated risk based on the formulas for the general population.
Conclusion: The excess cardiovascular risk among SLE patients varies substantially depending on the SLE-related risk factors, age, and traditional risk factors. Cardiovascular risk formulas based on individual data from SLE patients from the first year of their rheumatology followup may better estimate 10-year cardiovascular risk among SLE patients than the Framingham or AHA/ACC equations.

ACR 2019-Development of SLE CV Risk Equation-Abstract-Table1
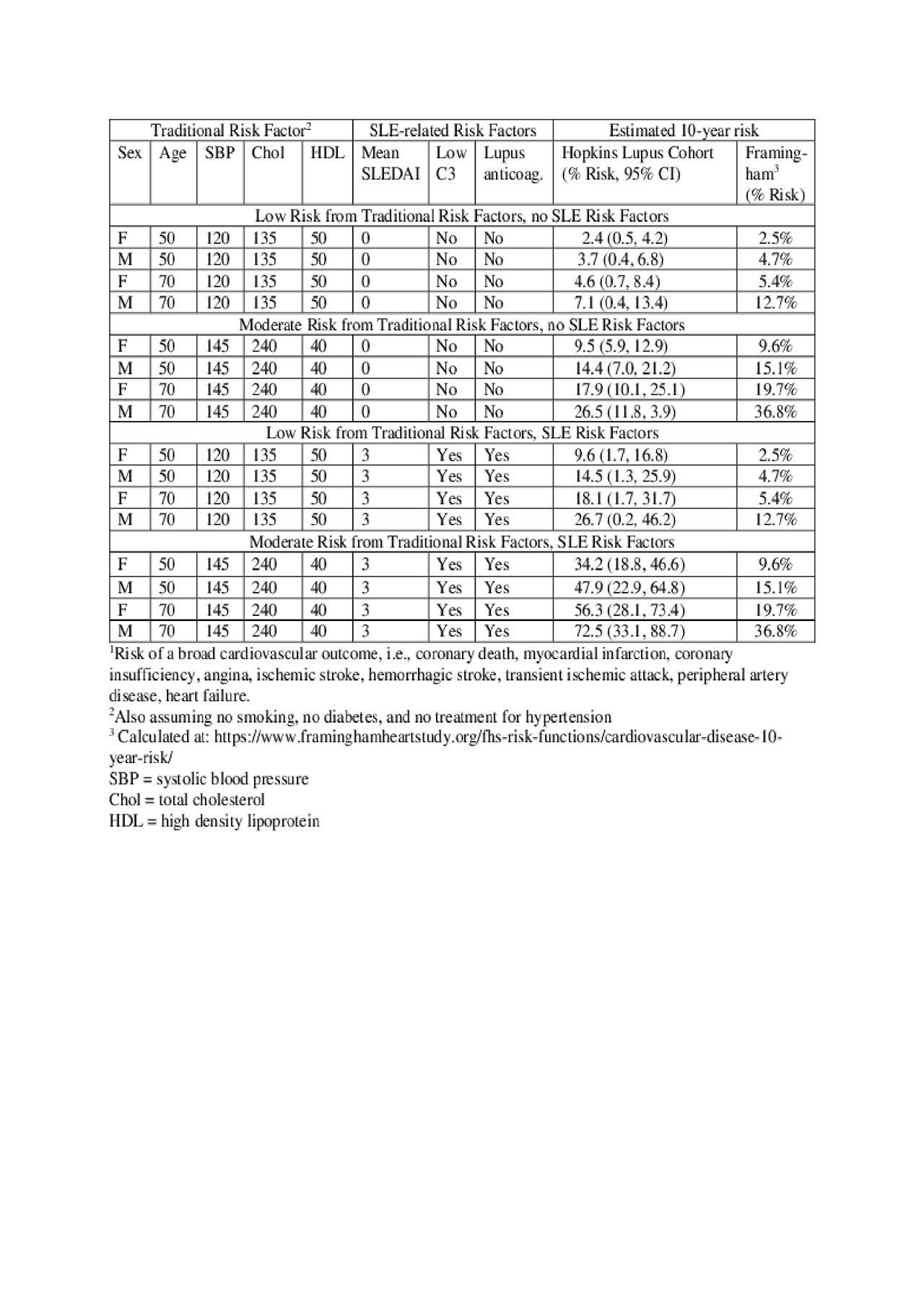
ACR 2019-Development of SLE CV Risk Equation-Abstract-Table2
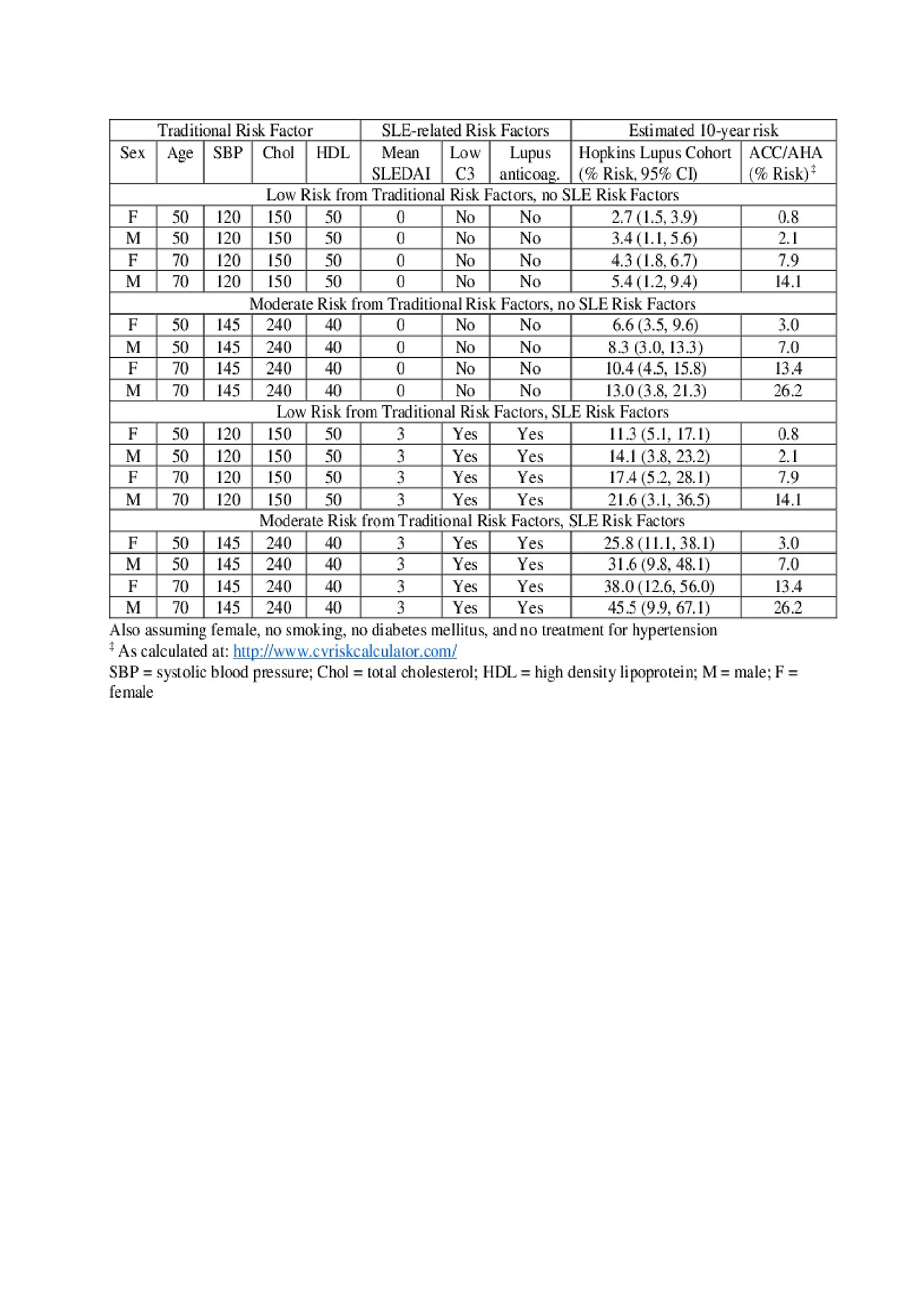
ACR 2019-Development of SLE CV Risk Equation-Abstract-Table3
To cite this abstract in AMA style:
Petri M, Barr E, Magder L. The Systemic Lupus Erythematosus Cardiovascular Risk Equation [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/the-systemic-lupus-erythematosus-cardiovascular-risk-equation/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-systemic-lupus-erythematosus-cardiovascular-risk-equation/