Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Adult-onset Still’s disease (AOSD) is a low prevalent disease with an unpredictable clinical course and variable prognosis. Sometimes, it requires biologic treatment in early phases of the pathology. A prognosis score has been described, which has never been applied in a Spanish case series.
Methods: Retrospective analysis realized in two University Hospitals. Clinical, laboratory, AOSD-related complications data, administered biologic treatments and number of deaths (AOSD related or not) were recorded. SS was applied at the onset of the disease development, assigning a point to each of the following 12 variables: fever, exanthema, pleuritis, pneumonitis, pericarditis, alteration of liver tests or hepatomegaly, splenomegaly, lymphadenopathy, odynophagia, leukocytosis > 15,000/mm3, myalgia and abdominal pain. A ≥ 7 score has been validated on other populations as the one which identifies the patients with high risk of complication. The relationship between prognosis score value and the next parameters was determined: clinical course, complications, biologic treatments administered and AOSD-related mortality. Sensitivity and Specificity of the SS value as a predictor of biologic treatment necessity was determined.
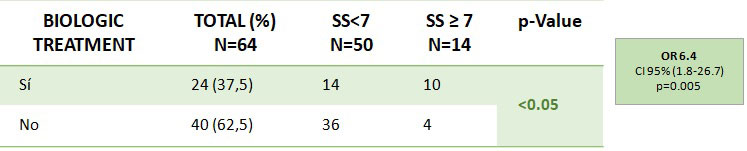
Results: Data from 64 patients was analyzed. Each patient was characterized for the presence of AOSD-related complications such as macrophage activation syndrome (MAS), myocarditis, renal involvement (tubulointerstitial nephritis, acute renal failure), secondary amyloidosis and AOSD-related death and all-causes death. After applying the SS, values of < 7 were obtained in 50 patients (78,13%) and of ≥7 in 14 patients (21,87%). MAS and renal involvement were significantly related with a score of ≥7 (Table 1). Myocarditis and secondary amyloidosis were not significantly associated with a high SS value. Even so, analyzing each case individually, it was found that they presented a score of ≥7, except for lung involvement. Biologic treatment requirement along the disease course was related to a score of ≥7 (OR: 6.4, IC95% [1.8%-26.7%]). Instead, it was not related to the different clinical patterns or the all-cause deaths. Related to sensitivity and specificity of the SS as a predictor of biologic treatment requirement, we observed that a value of ≥7 was the one which the highest area under the curve in the ROC curve (AUC = 0,629) in our population, with a sensitivity of 41,7% and specificity of 90%.
Conclusion: The prognosis score described by Pouchot et al could be useful to identify those patients with high risk of developing clinical complications and those who will need biologic treatment along the course of their disease. If a patient has a >7 score, the development of a macrophage activation syndrome or renal complications may be considered. Furthermore, the necessity of biologic treatment should be considered (Sensitivity: 41,7%, Specificity: 90%). It is necessary a higher number of patients to determine if the score could be useful to estimate the death risk related to AOSD complications.


To cite this abstract in AMA style:
Casafont-Solé I, Holgado S, Narváez J, Mora M, Roca J, Brandy-Garcia A, Mateo L, Martínez-Morillo M, Gifre L, Aparicio-Espinar M, Prior-Español �, Riveros-Frutos A, Sangüesa C, Camins-Fàbregas J, Nack A, Nolla J, Olivé-Marqués A. Adult-Onset Still’s Disease Prognosis Score: Clinical Patterns, Complications and Biologic Treatment [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/adult-onset-stills-disease-prognosis-score-clinical-patterns-complications-and-biologic-treatment/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/adult-onset-stills-disease-prognosis-score-clinical-patterns-complications-and-biologic-treatment/