Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: A self-report multi-dimensional health assessment questionnaire (MDHAQ) includes RAPID3 (routine assessment of patient index data), which is informative in all rheumatic diseases in which it has been studied. An electronic version of the MDHAQ (eMDHAQ) could offer several advantages, including completion at home rather than in the waiting area, as well as completion from any site between visits to report possible change in status and/or adverse events of a medication. Furthermore, the eMDHAQ includes 3 additional features beyond RAPID3 requiring computer software: a. MDHAQ/FAST3 (fibromyalgia assessment screening tool) – a 0–3 clue to fibromyalgia (FM) with 80% agreement with formal FM criteria; b. MDHAQ/MEMO60 (monitoring early medication outcomes) – using weekly remote electronic monitoring for 12 weeks after a new medication to analyze efficacy and adverse events; c.MDHAQ/LUCID (lifetime updatable clinical informatics database) – to provide medical history information in medical record format for physicians and to allow patients to save and update their medical history at a secure, HIPAA-compliant website for use with any doctor. We compared scores on an eMDHAQ vs paper version of MDHAQ at the same encounter, as well as patient preferences for the electronic vs paper MDHAQ.
Methods: All patients with all diagnoses complete a paper MDHAQ at all visits in the waiting area as part of routine clinical care. The MDHAQ includes 0-10 scores for physical function, pain and patient global visual analog scales (VAS), compiled into 0-30 RAPID3, as well as a 0–48 self-report painful joint count, and 0–60 symptom checklist. For this study, at the conclusion of the visit, the rheumatologist asked a patient if she/he would volunteer to complete an eMDHAQ on an iPad, indicating no problem if a patient declined. Patients who volunteered then completed an iPad eMDHAQ, with identical content to the paper MDHAQ. The patient also completed a 3-query questionnaire of 2 VAS concerning the value of the MDHAQ to the patient or the doctor (0= no value, 10= great value), and a query concerning preference for eMDHAQ vs paper MDHAQ or no preference. Test-retest reliability was examined by intraclass correlation coefficients (ICC).
Results: In 65 study patients, ICCs for physical function, patient global VAS, and RAPID3 were >0.9 indicating excellent reliability between the paper and Ipad eMDHAQ, and for pain, self-report painful joint count, and symptom checklist ≥0.75, indicating good reliability. The mean ratings for the value of MDHAQ were 8.85/10 to the patient and 8.88/10 to the doctor. Among the 65 patients, 43 (66%) preferred the eMDHAQ, 7 (11%) the paper MDHAQ, and 15 (23%) indicated no preference.
Conclusion: An eMDHAQ provides similar results to a paper MDHAQ. Most patients preferred the eMDHAQ to paper, although about 20% of patients likely will require a paper MDHAQ. An eMDHAQ offers remote completion before and/or between visits, and to report problems and/or adverse events, as well as unique electronic features. eMDHAQ is designed to interface with any electronic medical record (EMR), although that requires interaction with the EMR vendor, which may be difficult. The eMDHAQ appears useful independent of the EMR.
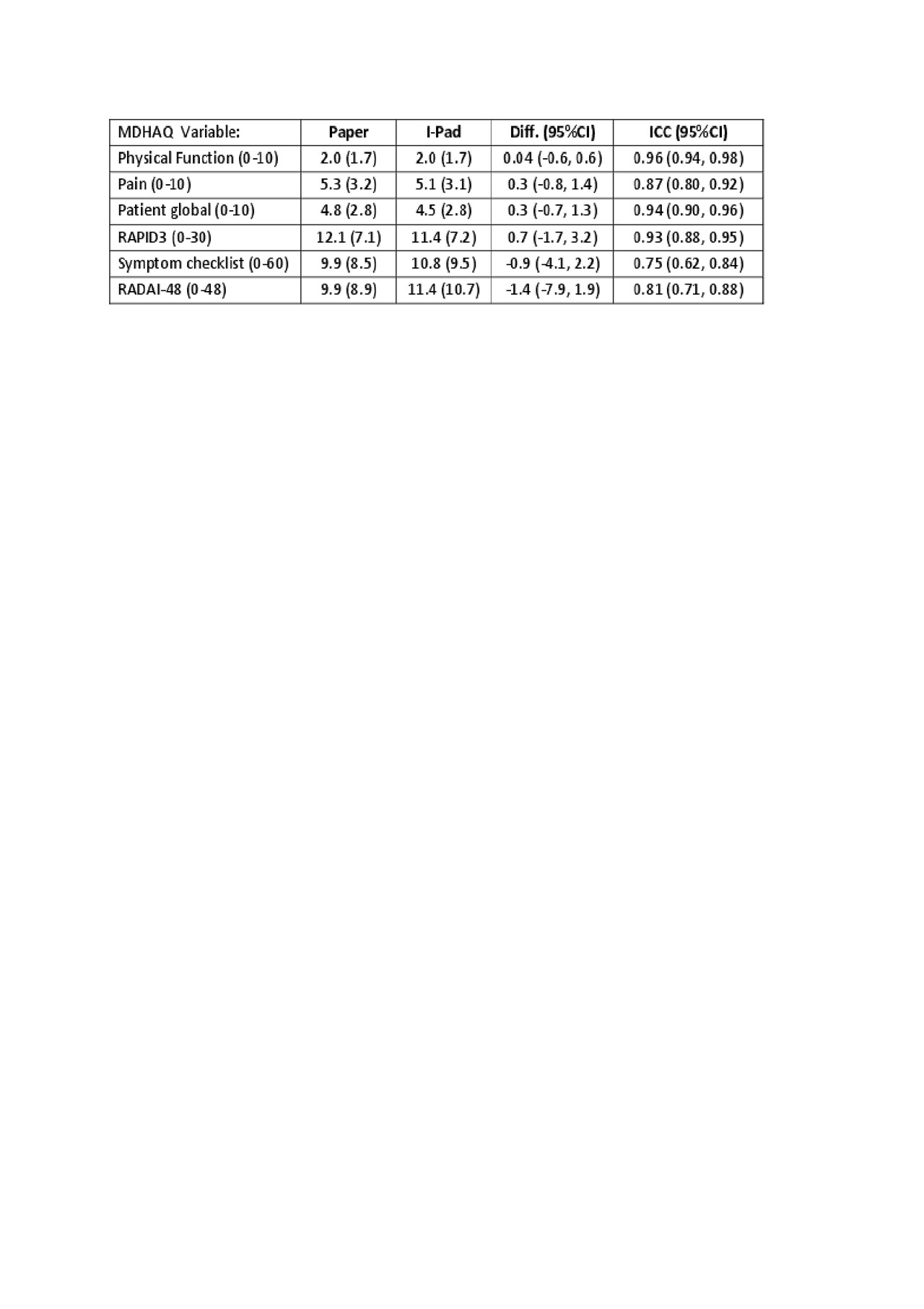
electronic table
To cite this abstract in AMA style:
Pincus T, Riad M, Obreja E, Lewis C, Castrejon I. Patient Preference for an Electronic MDHAQ/RAPID3 (Multidimensional Health Assessment Questionnaire/ Routine Assessment of Patient Index Data), Which Gives Similar Results Compared to a Paper Version [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/patient-preference-for-an-electronic-mdhaq-rapid3-multidimensional-health-assessment-questionnaire-routine-assessment-of-patient-index-data-which-gives-similar-results-compared-to-a-paper-version/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patient-preference-for-an-electronic-mdhaq-rapid3-multidimensional-health-assessment-questionnaire-routine-assessment-of-patient-index-data-which-gives-similar-results-compared-to-a-paper-version/