Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose:
There are multiple instruments to measure rheumatoid arthritis disease activity using various patient, lab or physician parameters. Since the RAPID3 has been published, there have been a few studies re-evaluating the target scores based on clinical experience. We re-evaluated the RAPID3 value for low disease activity and comparing it to two well established instruments approved by ACR, namely CDAI and SDAI.
Methods:
A retrospective observational study was done from a single practice database in a community-based rheumatology clinic. Random visits from 345 patients with a diagnosis of rheumatoid arthritis who had documented RAPID3, CDAI and SDAI were studied. Baseline patient demographics, RAPID3, CDAI, SDAI, tender count, swollen count, physician global, pain scale, patient global function was collected. Receiver operator curves (ROC) were created using either low CDAI ( CDAI <=10.0 ) or low SDAI ( SDAI<=11.0 ) and a complete sensitivity/specificity report was analyzed using random patient visits.
Results:
Study population consisted of 345 patients with documented RAPID3 scores with a mean of 10.19 (0-30) and SD 6.89. The comparison of RAPID 3 with low CDAI, it yielded an area under the curve of 0.84 on the ROC (95% CI 0.80-0.88) ( Figure 1) with a sensitivity of 74.21% and specificity of 83.87% for a RAPID3 score of 8.0 (0-30). Similarly, in comparison with low SDAI, it yielded an area under curve of 0.84 on the ROC (95% CI 0.79 – 0.87) with a sensitivity of 74.69% and specificity of 83.06% for a RAPID3 score of 8.2 (0-30). If we reconsider a low disease activity score of 8.0 on the RAPID3, approximately 10% of this patient population were misclassified.
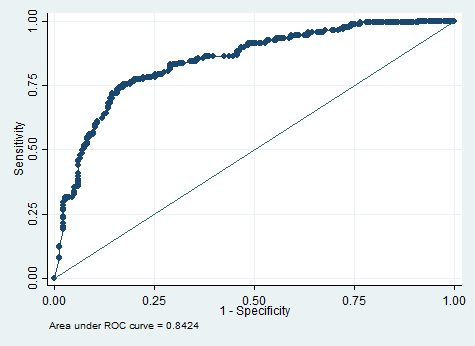
Figure 1, Reciever Operator Curve RAPID3 vs low CDAI
Conclusion:
In this cohort, low CDAI and SDAI disease activity were found to be correlated to a higher RAPID3 score cut off. Currently, CDAI low disease activity is defined as >2.8-10, SDAI low disease activity as 3.3-<11 and RAPID3 low disease activity as >3.0-6.0. Using the current low disease activity cut off, our treat to target goal may be misclassifying these patients from low to moderate disease activity thereby overtreating them. We propose that the definition of low disease activity for the RAPID 3 to be <8.0 on a 0-30 scale. Further studies comparing these findings as well as other cut off ranges using larger number of patients are required to substantiate this study.
To cite this abstract in AMA style:
Tiwari V, Maheshwari A, Dheer S, Bergman MJ. Proposal to Re-Evaluate the Definition of Low Disease Activity in Routine Assesment of Patient Index Data 3 (RAPID3) in Rheumatoid Arthritis Patients [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/proposal-to-re-evaluate-the-definition-of-low-disease-activity-in-routine-assesment-of-patient-index-data-3-rapid3-in-rheumatoid-arthritis-patients/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/proposal-to-re-evaluate-the-definition-of-low-disease-activity-in-routine-assesment-of-patient-index-data-3-rapid3-in-rheumatoid-arthritis-patients/