Session Information
Date: Sunday, October 21, 2018
Title: Systemic Lupus Erythematosus – Clinical Poster I: Clinical Manifestations and Comorbidity
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
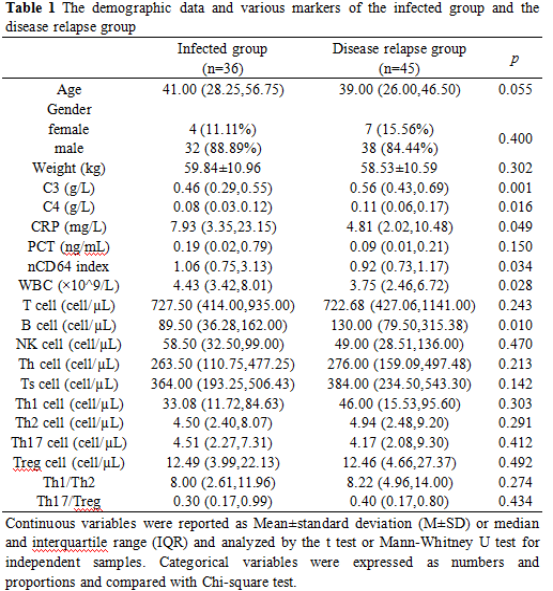
Background/Purpose: Patients with Systemic lupus erythematosus (SLE) are prone to bacterial infection owing to disease activity, abnormal immune function and long-term immunosuppressive therapy. Differentiating bacterial infection from disease relapse in SLE is challenging based on clinical signs and symptoms due to similar clinical presentation. Microbial culture is the gold standard for diagnosing bacterial infection, but it is time-consuming and the positive culture ratio is low. The role of several biomarkers including C-reactive protein (CRP), procalcitonin (PCT) and white blood cell count (WBC) for diagnosing bacterial infection is controversial. The study is aimed at evaluating the significance of neutrophil CD64 (nCD64) index, complement C3, complement C4, CRP, PCT, WBC, lymphocyte subsets, CD4+T subsets and their combination in differentiating bacterial infection from disease relapse in SLE.
Methods: Thirty-six hospitalized SLE patients with bacterial infection and 45 with lupus flare without infection were retrospectively studied. Bacterial infection was proven by positive cultures or typical clinical symptoms and signs combined with positive response to antibiotics. Lupus flare was considered as three points greater than the patient’s previous SLEDAI. C3, C4, CRP and PCT were detected by immunoturbidimetry. Lymphocyte subpopulations, CD4+T subsets and nCD64 index were measured by flow cytometry. WBC was detected by blood cell analyzer.
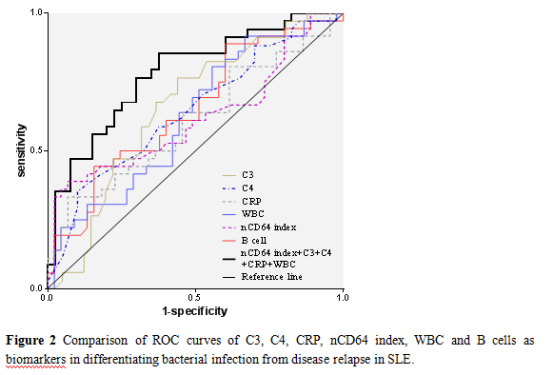
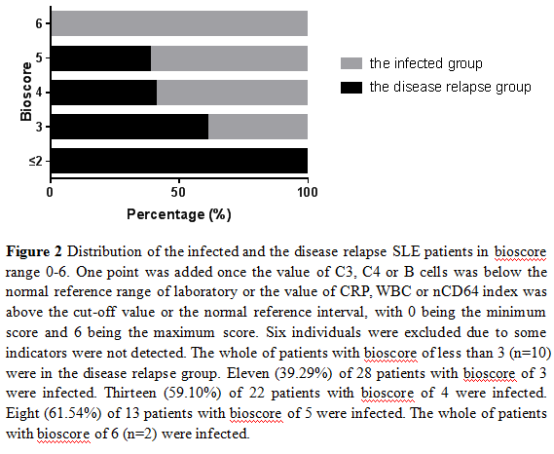
Results: The levels of nCD64 index (p=0.034), CRP (p=0.049) and WBC (p=0.028) were significantly higher in the infected group and C3 (p=0.001), C4 (p=0.016) and B cells (p=0.010) were lower. The areas under the receiver operating characteristic (ROC) curves (AUC) for the above six biomarkers had no significant difference [nCD64 index: 0.619 (CI 0.504-0.724), CRP: 0.608 (CI 0.492-0.715), WBC: 0.625 (CI 0.510-0.730), C3: 0.658 (CI 0.540-0.764), C4: 0.646 (CI 0.526-0.754), B cells: 0.652 (CI 0.538-0.754)] and the best combination was nCD64 index, CRP, WBC, C3 and C4. The bacterial infection rate in patients with bioscore ≤ 2, 3, 4, 5 and 6 were 0.00%, 39.29%, 59.10%, 61.54% and 100.00%, respectively.
Conclusion: The combination of nCD64 index, C3, C4, CRP, WBC and B cells in a bioscore is useful to diagnose bacterial infection in SLE.
To cite this abstract in AMA style:
Feng M, Liang Z, Zhao X, Gao C, Luo J. Peripheral Neutrophil CD64 Index Combined with Biomarkers Improves the Ability of Diagnosing Bacterial Infection in Patients with SLE [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/peripheral-neutrophil-cd64-index-combined-with-biomarkers-improves-the-ability-of-diagnosing-bacterial-infection-in-patients-with-sle/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/peripheral-neutrophil-cd64-index-combined-with-biomarkers-improves-the-ability-of-diagnosing-bacterial-infection-in-patients-with-sle/