Session Information
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose:
Cognitive function may change over time in patients with SLE, and cognitive function trajectories (CFTs) have not well been studied. This is the first study to identify CFTs in SLE and their correlates.
Methods:
Data were from the University of California San Francisco Lupus Outcomes Study, in which participants are followed longitudinally via annual telephone surveys. The Hopkins Verbal Learning Test-Revised (HVLT-R; measures verbal memory) was administered in years 2-7 and the Controlled Oral Word Association Test (COWAT; verbal fluency) in years 4-7, providing up to 6 and 4 years of observation, respectively. Individuals with at least 2 assessments were included in analysis. Age- and education-stratified z-scores were derived for HVLT delayed recall and COWAT.
Proc Traj (SAS) was used to identify group-based trajectory models. One model each was fitted for the HVLT-R and COWAT. To select the best model, models with 2-5 trajectories were examined by graphic shapes, number of patients in each group, and model fitting statistics according to Baysian Information Criterion. Separate univariate/multivariable logistic regression analyses (for HVLT-R and COWAT) were then performed to look for factors at baseline associated with CFT, including sex, ethnicity, disease duration, renal problems, treatments, fatigue, depressive symptoms (CESD), and self-reported disease activity.
Results:
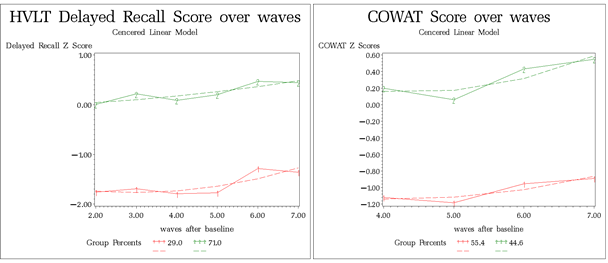
815 patients (92.4% female) with mean age 34.5±13.3 years at SLE diagnosis were studied. 761 and 658 individuals had at least 2 HVLT-R and COWAT scores, respectively. Two CFTs were identified for each measure (see Figure): persistently low (29% in HVLT-R, 55% in COWAT) and persistent normal (71% in HVLT-R, 44.6% in COWAT). In multivariable analyses, persistently normal HVLT-R was associated with Caucasian race; renal problems, intravenous glucocorticoids use in the prior year, and higher CESD scores were associated with persistently low HVLT-R (Table). Persistently normal COWAT was associated with longer disease duration, while higher CESD score was associated with persistently low COWAT.
Conclusion:
Cognitive function followed particular trajectories over time in SLE, with some patients having persistently low scores while others had normal scores. Depressive symptoms were associated with persistently low function in both measures. Other factors associated with persistently low function were measure-specific. Additional longitudinal studies including more nuanced measures of cognitive function are needed to further explore long-term patterns of cognitive function in SLE.
|
Table. Baseline factors associated with better cognitive function trajectories in univariate and multivariate analysis |
||||
|
|
HVLT-R delayed recall |
COWAT |
||
|
|
Univariate |
Multivariate |
Univariate |
Multivariate |
|
Female |
1.3 (0.7, 2.3) |
— |
1.0 (0.5, 1.8) |
— |
|
Caucasian |
1.6 (1.1, 2.2) |
1.5 (1.02, 2.2) |
1.3 (0.9, 1.9) |
— |
|
Disease duration, year |
1.0 (0.98, 1.02) |
— |
1.02 (1.0, 1.03) |
1.02 (1.001, 1.04) |
|
Renal problems |
0.5 (0.4, 0.8) |
0.6 (0.4, 0.9) |
0.8 (0.5, 1.1) |
— |
|
Smoking, ever |
0.8 (0.6, 1.2) |
— |
1.3 (0.9, 1.7) |
— |
|
Oral glucocorticoids during baseline year |
0.8 (0.6, 1.1) |
— |
0.8 (0.6, 1.1) |
— |
|
Intravenous steroids during baseline year |
0.4 (0.2, 0.8) |
0.5 (0.2, 0.4) |
0.9 (0.5, 1.7) |
— |
|
Plaquenil use |
0.8 (0.6, 1.1) |
— |
1.2 (0.9, 1.7) |
— |
|
CESD score |
0.96 (0.95, 0.97) |
0.97 (0.96, 0.98) |
0.98 (0.97, 0.99) |
0.98 (0.97, 1.0) |
|
Tabled values are odds ratios (95% confidence intervals). |
||||
To cite this abstract in AMA style:
Touma Z, Su J, Katz PP. Longitudinal Assessment of Cognitive Function in SLE: Identification of Trajectories [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/longitudinal-assessment-of-cognitive-function-in-sle-identification-of-trajectories/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/longitudinal-assessment-of-cognitive-function-in-sle-identification-of-trajectories/