Session Information
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Patients and physicians commonly differ in their evaluations of rheumatoid arthritis (RA) activity. However, clinically meaningful thresholds for such discordance or validation of their ability to optimally predict clinical and functional outcomes are lacking. We used an unbiased clustering approach to classify cases based on patient (PGA) and physician/evaluator (EGA) global assessments of RA activity. We first examined whether such an approach could generate distinct patient groupings with diverse clinical phenotypes. We subsequently explored whether this approach could explain a higher variance in clinical and functional parameters of interest compared to traditional discordance definitions.
Methods: We performed latent class cluster (LCC) analysis in 538 patients with established RA to identify patient subgroups based on PGA and EGA ratings (measured on 10-cm visual analogue scales). Conventional discordance definitions included a continuous score (PGA-EGA) as well as a threshold-based one; with the latter, patients were classified into three groups: concordant (PGA-EGA within ± 3cm), positively discordant (PGA-EGA ³ 3cm) and negatively discordant (PGA-EGA ² -3cm). We used R2 values to compare the explanatory power of regression models using LCC-generated solution or conventional discordance definitions to predict outcomes of interest.
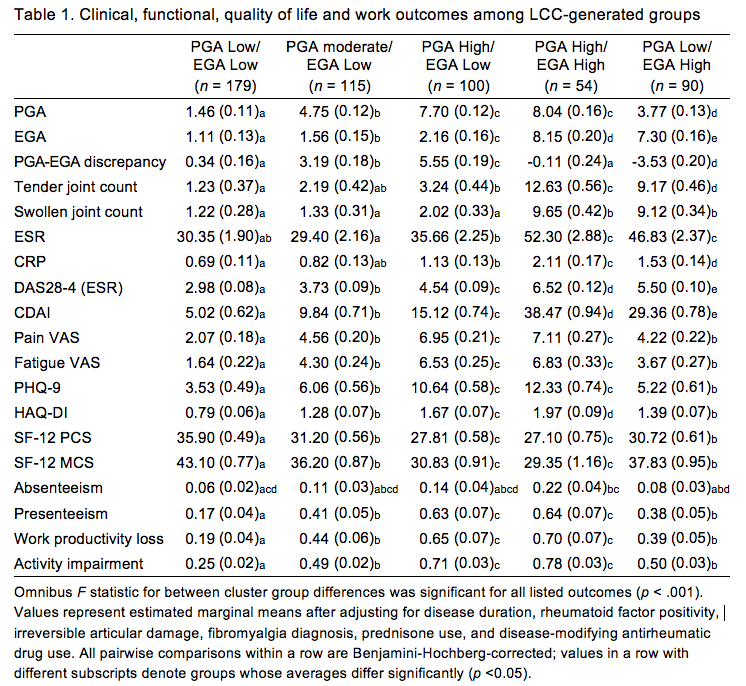
Results: LCC analysis yielded a five-group solution (Fig 1A). Groups were distinct and reflected different pairings of PGA and EGA scores: (1) Low PGA/Low EGA (33%); (2) Moderate PGA/Low EGA (21%); (3) High PGA/Low EGA (19%); (4) High PGA/High EGA (10%); and (5) Low PGA/High EGA (17%). Classification accuracy was 98.3%. ANCOVA confirmed differences in characteristics among LCC groups (Table 1). The High PGA/High EGA group fared worst overall, with patient outcomes similar or worse than the High PGA/Low EGA group and clinician-evaluated indices comparable to or worse than the Low PGA/High EGA group. The explanatory power of the LCC-based solution significantly outperformed conventional discordance definitions predicting all measured outcomes (Fig 1B).
Conclusion: Our findings highlight the validity and advantages of an LCC approach in quantifying the relationship between patient-physician global activity assessments, based on two simple measures collected in routine practice. LCC-generated groups differed significantly across clinical, functional and quality of life outcomes, and identified patients in greatest need of adjunctive treatments targeting pain, fatigue and psychological distress.

To cite this abstract in AMA style:
Karpouzas G, Ormseth S. A Cluster Analysis Approach to Patient-Physician Discordance in Rheumatoid Arthritis Activity Evaluations Optimally Differentiates and Predicts Clinical, Functional and Quality of Life Outcomes [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/a-cluster-analysis-approach-to-patient-physician-discordance-in-rheumatoid-arthritis-activity-evaluations-optimally-differentiates-and-predicts-clinical-functional-and-quality-of-life-outcomes/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-cluster-analysis-approach-to-patient-physician-discordance-in-rheumatoid-arthritis-activity-evaluations-optimally-differentiates-and-predicts-clinical-functional-and-quality-of-life-outcomes/