Session Information
Date: Monday, November 6, 2017
Title: Health Services Research Poster II: Osteoarthritis and Rheumatoid Arthritis
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: The rising prevalence of heart failure (HF) in the general population and associated increased hospitalization costs is a major public health problem. There is a 2-fold increased risk of HF in rheumatoid arthritis (RA) compared to the general population. Little is known about hospitalization rates in patients with RA and HF. We aimed to compare the frequency of and trends in hospitalizations following HF diagnosis in patients with and without RA during 1987-2015.
Methods: The study included a retrospectively identified population-based cohort of patients with incident HF and prior RA (age≥18 years, 1987 ACR criteria) and a comparison cohort of incident HF patients without RA matched 3:1 on age, sex, and year of HF diagnosis. Hospitalizations at the time of HF diagnosis were excluded from analyses. All subjects were followed until death, migration, or 1/1/2015. Person-years methods and rate ratios (RR) from Poisson regression models were used to compare hospitalization rates between the groups. Generalized linear models were used to analyze the length of stay (LOS).
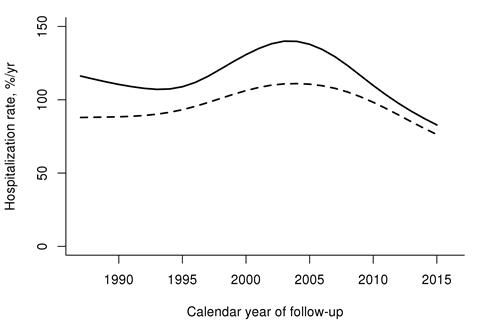
Results: The study included 212 patients with RA (mean age at HF diagnosis 78.3 years; 68% female) and 636 non-RA patients (mean age at HF diagnosis 78.6 years; 68% female). The hospitalization rate following HF diagnosis was higher in RA vs non-RA patients (RR 1.16; 95%CI 1.08-1.25). This difference may be decreasing after 2010 (Figure). The magnitude of the increase was similar in both sexes and across all ages. In patients with available echocardiography, HF with preserved ejection fraction (HFpEF) was not different in RA (57%) vs non-RA (51%; p=0.3). Patients with RA and HF with reduced ejection fraction (HFrEF, RR 1.65; 95%CI 1.29-2.09) but not those with HFpEF (RR 0.80; 95%CI 0.63-1.01) had significantly more hospitalizations than non-RA patients. Following HF diagnosis, RA patients were more likely to be hospitalized for non-cardiovascular causes (RR 1.26; 95%CI 1.14-1.39), but not for HF (RR 0.96; 95%CI 0.76-1.21) or other cardiovascular causes (RR 0.99; 95%CI 0.81-1.20) compared to the non-RA patients. There was no overall difference in hospital LOS in RA vs non-RA patients after HF diagnosis (mean of 5.6 vs 5.3 days, respectively, p=0.31). LOS was higher in earlier years in RA than non-RA and declined faster in RA than non-RA over time, with similar LOS in both groups in recent years (interaction p=0.019). Readmission rates within 30 days of prior discharge were similar in RA and non-RA (p=0.14).
Conclusion: Hospitalization rate following HF diagnosis was 16% higher in RA than in non-RA patients regardless of sex and age. This increased hospitalization risk was mostly among patients with RA who had HFrEF rather than HFpEF, and was predominantly due to non-cardiovascular causes. Increased complexity of management of patients with comorbid RA may play a role in more frequent hospitalizations in the RA cohort.
To cite this abstract in AMA style:
Myasoedova E, Matteson EL, Achenbach SJ, Davis JM III, Setoguchi S, Gabriel SE, Crowson CS. Trends in Hospitalizations Following Heart Failure Diagnosis in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/trends-in-hospitalizations-following-heart-failure-diagnosis-in-rheumatoid-arthritis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/trends-in-hospitalizations-following-heart-failure-diagnosis-in-rheumatoid-arthritis/