Session Information
Session Type: ACR Poster Session B
Session Time: 9:00AM-11:00AM
Background/Purpose: There has been increasing interest in hip morphology as a risk factor for OA. There is a need for frequency estimates in the general population (Dickenson OAC 2016). We aimed to provide a description of these measures in a well-characterized community-based cohort.
Methods: This cross-sectional analysis involved data collected during 1991-1997 from the Johnston County OA Project. Hip morphology measures were defined using OxMorf software (Oxford, UK). Radiographic hip OA (rHOA) was defined, at the participant level, if at least one hip had Kellgren-Lawrence grade 2 or more. Descriptive means and 95% confidence intervals for hip measures were obtained from unadjusted regression and logit models, as appropriate, using GEE to account for within-participant hip correlation, stratified by sex and rHOA status; comparisons were qualitative.
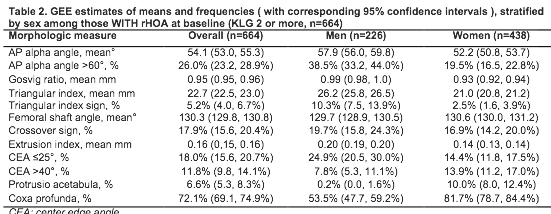
Results: Complete data were available for 4519 hips from 2263 individuals, mean age 64 years, mean BMI 29 kg/m2, 30% African American, 39% male. Several measures although different by sex, did not differ substantially between those with and without rHOA (triangular index height, femoral shaft angle, extrusion index, coxa profunda). Results for those without rHOA are shown in Table 1. Only crossover sign (~20%) and lateral center edge angle (CEA) <=25 degrees (~25%) were more frequently seen in the non-rHOA compared with the rHOA group. Pathologic AP alpha angles over 60 degrees were seen in 20% of men and 7% of women, while only around 1% had a triangular index sign, both signs of cam-type morphology. About a quarter had CEA <=25 degrees, consistent with mild dysplasia. In contrast, several measures were higher in those with rHOA in at least one hip (Table 2), including AP alpha angle, Gosvig ratio, the proportion with triangular index sign, CEA >40 degrees, and protrusio acetabuli. AP alpha angle > 60 degrees was twice as common in those with rHOA (26% overall; 39% of men, 20% of women) versus those without, and 5% had a triangular index sign. Other measures suggestive of cam type deformity (continuous alpha angle and Gosvig ratio) were also higher compared to the non-rHOA group. CEA > 40 degrees was about twice as frequent among men and women with rHOA versus those without. Protrusio was twice as frequent among women with versus women without rHOA, but was rare in men.
Conclusion: One out of 5 men without rHOA, and 2 out of 5 with rHOA, have a pathologic AP alpha angle in this sample. Radiographic assessment of most measures is confounded by morphologic changes due to rHOA; however, some were not. Both cam-type (alpha angle, Gosvig ratio) and pincer-type (protrusio, CEA >40 degrees) were more common in those with rHOA. 
To cite this abstract in AMA style:
Nelson AE, Raveendran R, Stiller JL, Alvarez C, Renner JB, Schwartz TA, Arden NK, Jordan JM. Description of Radiographic Hip Measurements By OA Status in a Large Community-Based Study of African American and White Men and Women [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/description-of-radiographic-hip-measurements-by-oa-status-in-a-large-community-based-study-of-african-american-and-white-men-and-women/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/description-of-radiographic-hip-measurements-by-oa-status-in-a-large-community-based-study-of-african-american-and-white-men-and-women/