Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Pulmonary hypertension (PH) is the leading cause of scleroderma related deaths and is often detected late in the disease course. Early identification of patients with PH will lead to earlier treatment and may improve survival. The purpose of this study is to evaluate if a positive EE predicts future development of PH in a high-risk cohort of scleroderma patients.
Methods: This study included 100 scleroderma patients with features placing them at increased risk for pulmonary hypertension, including dyspnea on exertion, DLCO <60% of predicted, FVC <60% of predicted, FVC%/DLCO% >1.6, or resting right ventricular systolic pressure (RVSP) 30-50 mm Hg. In this prospective cohort study, all patients had baseline EE performed by the standard Bruce stress echocardiogram protocol with re-measurement of RVSP within 1 minute of stopping exercise. A positive EE was defined as an increase of at least 20 mmHg in the RVSP with exercise. All patients had at least one repeat echocardiogram at least one year after baseline EE. Patients were followed per standard of care and right heart catheterization (RHC) was performed in patients with a positive EE result or if PH was suspected based on symptoms. Time to follow up was defined as months to the development of resting PH, or in patients who did not develop PH, months from initial EE to the last echocardiogram.
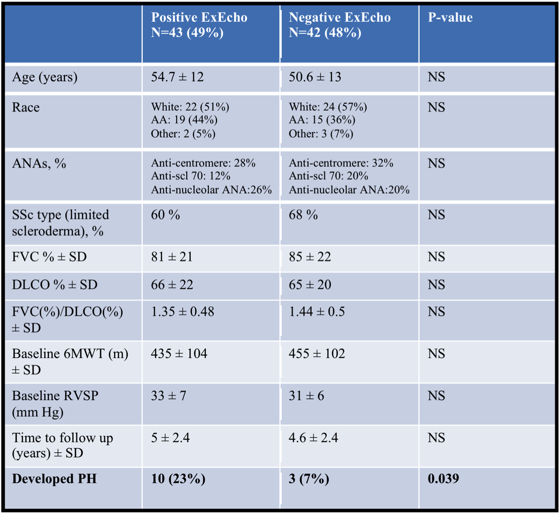
Results: In our patient population, 12 patients were excluded as they did not have a repeat echocardiogram and 3 additional patients were excluded as they were being treated for exercise PH at the time of EE. Table 1 shows in the remaining cohort, 43 patients had a positive EE and 42 patients had a negative EE. There were no clinical demographic differences or differences in cardiopulmonary parameters between groups. In the positive EE cohort, 10 patients (23%) developed resting PH on RHC, a mean of 4 years after EE (4 with pulmonary arterial hypertension (PAH), 5 with pulmonary venous hypertension (PVH), and 1 with pulmonary hypertension associated with lung fibrosis (PH-ILD), whereas in the negative EE group, only 3 (7%) patients developed pulmonary hypertension (1 PAH, 2 PVH) (p=0.039). Of the remaining 33 patients with positive EE who did not develop resting PH, most (51%) patients continued to have a positive EE, with a mean of 5.3 years of follow up. This included 18 patients who had exercise induced pulmonary hypertension as documented on RHC, but who did not develop worsening symptoms, or changes on the echocardiogram over time.
Conclusion: While a positive EE does predict the future development of resting PH, it is not necessarily PAH, even in high-risk scleroderma patients. PVH also is associated with a positive EE. Many patients with a positive EE may have a persistently positive exercise echocardiogram without progression to resting pulmonary hypertension. A persistently negative EE may identify patients at low risk for future PH. Table 1:
To cite this abstract in AMA style:
Quinn KA, Kuru T, Wappel S, Steen VD. Exercise Echocardiography Predicts Future Development of Pulmonary Hypertension in a High-Risk Cohort of Scleroderma Patients [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/exercise-echocardiography-predicts-future-development-of-pulmonary-hypertension-in-a-high-risk-cohort-of-scleroderma-patients/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/exercise-echocardiography-predicts-future-development-of-pulmonary-hypertension-in-a-high-risk-cohort-of-scleroderma-patients/