Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with autoimmune conditions have higher rates of pneumococcal disease and they are often immunosuppressed. In 2014, the Advisory Committee on Immunization Practices issued new guidelines recommending vaccination with the 13-valent pneumococcal conjugate vaccine (PCV-13) for immunosuppressed patients. However, only 12% of patients on immunosuppression were vaccinated at our academic referral center. Our aim was to use the Institute for Healthcare ImprovementÕs Model for Improvement to increase the PCV-13 vaccination rate from 12% to 40%.
Methods: Plan-Do-Study-Act (PDSA) methodology was used over 3 cycles within a large rheumatology practice. Patients were eligible for vaccination if they were prescribed disease modifying antirheumatic drugs (DMARDs), biologic agents, or prednisone. Prior to the start of the intervention, vaccination rates were reviewed between 5/1/2014 and 3/1/2015. PDSA Cycles included: (1) Investigator-led educational session for providers regarding risks of pneumococcal disease and benefits of new vaccine (3/1/15 to 5/1/15); (2) Medical assistant (MA) training, utilization of the electronic medical record (EMR) by messaging patients if there was no documentation of their vaccination status prior to visit (5/1/15 to 7/1/15) (3) Creation of a paper form for MAs to complete and indicate patient eligibility followed by MAs writing electronic pended orders, if appropriate. (7/1/15-4/1/16) On a quarterly basis, vaccination rates were abstracted from the EMR (Apex and Clarity) and vaccination rates were tracked using p-charts.
Results: 9 rheumatology fellows, 11 faculty members, 1 nurse practitioner and 9 medical assistants participated in the quality improvement activity. Prior to the intervention, 12% patients had received a PCV-13 vaccination in clinic over a 10-month period. After the third PDSA cycle, over 52% of eligible patients received a PCV-13 vaccination (see Figure).
Conclusion: Targeted education for clinicians and medical assistants in conjunction with using EMR tools for patient reminders and MA-generated orders increased rates of pneumococcal vaccination from 12% to 52% in our large academic rheumatology practice. Ultimately, paper reminders for providers and pended orders by the MAs, in addition to previous interventions, resulted a sustained increase in vaccination rates over a 9-month period without further interventions. Future work will include surveying stakeholders and identifying remaining barriers to vaccination to further increase vaccination rates. 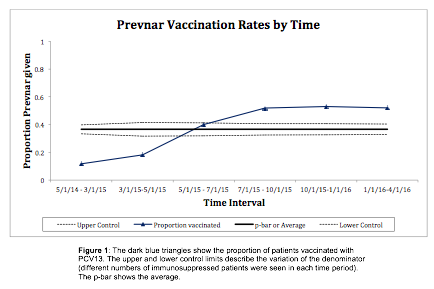
To cite this abstract in AMA style:
Bays A, Nayak RR, Murray S, Young D, Schmajuk G, Yazdany J, Gross A. Improving Pneumococcal Vaccination Rates for Immunosuppressed Patients in an Academic Rheumatology Clinic [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/improving-pneumococcal-vaccination-rates-for-immunosuppressed-patients-in-an-academic-rheumatology-clinic/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-pneumococcal-vaccination-rates-for-immunosuppressed-patients-in-an-academic-rheumatology-clinic/