Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Title: Telerheumatology: A Technology Not
Appropriate For All
Background/Purpose: Access to Rheumatology care in New Hampshire (NH) and
Vermont (VT) is limited, as a large proportion of the population lives in rural
areas (60%) with limited resources. Telerheumatology services developed at Dartmouth-Hitchcock Medical Center (DHMC)
brings care to these rural regions and improves access. Our previous
work identified two issues with telerheumatology: 1) the
quality of the patient presenter and 2) the appropriateness of the patient for
a telerheumatology visit. We want to systematically assess the patient
and provider experience to improve the quality of care delivered via telerheumatology.
Methods: As part of a quality improvement initiative we performed an IRB-exempt
retrospective review of the charts for patients seen in the telerheumatology
clinic at DHMC from October 2011 to December 2014. We also interviewed the
participants: including providers, presenters and patients regarding their
experience of care. We assessed both patient and provider satisfaction with the
experience. We developed a web based educational series on rheumatic disease,
including MSK examination, for the presenter. We used descriptive statistics to
summarize our findings.
Results:
Between October 2011 and December 2014, 176 patients were seen via telerheumatology between two clinical sites over the course
of 244 patient visits. The
top diagnosis for patients seen was inflammatory arthritis (n=156, 63.9%).
66.4% of the patients were on high risk medications including: steroids,
biologics (infusion and injectable), and DMARDs. Providers filled out surveys
on 9 visits for 70 patient encounters and found that 19% of patients (13) were inappropriate for the visit type for
two main reasons: diagnosis unclear or diagnosis too complex. Telerheumatology afforded patients shorter travel distances
and travel related money savings. 94% of patients were satisfied with the
remote site staff and treating providers, and 73% of them would like to be seen
via telerheumatology again. We previously provided
presenter education which had no impact on the provider perceived quality of
the visit.
Conclusion: The use of telerheumatology has successfully
increased access to rheumatology care for patients in rural regions of NH and
VT allowing for shorter travel and cost savings. 19% of the patient visits
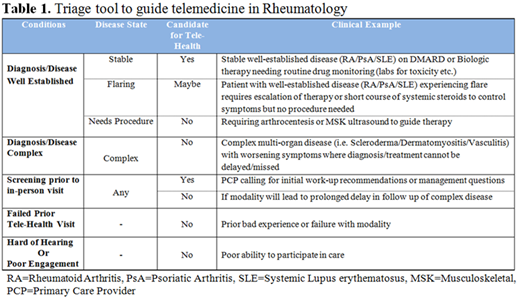
reviewed were inappropriate for the visit modality. This evaluation was performed in a setting
without any pre-visit screening, which we believe could be an opportunity to
triage patients to the appropriate visit modality. We propose a triage mechanism (Table 1) to pair
patients appropriately with the telerheumatology visit
type to ensure an overall high quality experience for patients and providers in
the future.
To cite this abstract in AMA style:
Kulcsar Z, Albert D, Ercolano E, Mecchella J. Telerheumatology: A Technology Not Appropriate for All [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/telerheumatology-a-technology-not-appropriate-for-all/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/telerheumatology-a-technology-not-appropriate-for-all/