Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Magnetic resonance imaging (MRI) captures joint inflammation and damage in gouty arthropathy and can also reveal tophi. We have investigated reader reliability for scoring the MRI features of gout and have explored the association between erosions and tophi. We have also compared MRI with Dual Energy Computed Tomography (DECT) scans of the same region, to define sensitivity and specificity of MRI for tophi.
Methods: 3T MRI scans of the dominant wrist were obtained in 40 patients with severe, longstanding gout. The median/range patient age was 55.5 years (29 – 70), disease duration 17 years (1 – 42), serum urate 0.39mmol/L (0.2 – 0.69), 70% were of Polynesian/Maori ethnicity, and 85% had a history of tophi. All scans were scored separately (blinded) by 2 radiologist readers, for synovitis, bone oedema, erosions and tophi at 15 carpal sites including the bases of 1-5 metacarpals using RAMRIS criteria. Inter-reader reliability for scoring all features was determined. In a subgroup of 10 patients, DECT scans were obtained of the same region and scored by a separate reader for tophi at the same sites (or in adjacent soft tissue).
Results: Reliability was high between MRI readers for bone erosion and tophus size (ICCs 0.77 [95%CI: 0.71-0.87] and 0.71 [0.52, 0.83] respectively); and was moderate for synovitis and bone oedema (ICCs 0.62 [95%CI: 0.34-0.80] and 0.60 [0.36, 0.77] respectively). Concordance between readers for erosions was 82%, for all tophi was 85% and for tophi > 5mm was 93%. When a stringent analysis was performed (features were only counted if scored by both observers = “2-reader MRI”), 63% of patients were positive for bone erosions, 30% for bone oedema, 28% for tophi, 25% for tophi > 5mm and 61% for synovitis. The Odds ratio (OR) for tophus coexisting with erosion on MRI was 13.0 [95% CI: 1.5 – 113] when all sites were treated as independent and 2.9 [95% CI: 1.6 – 4.2] when the patient effect was factored in. When MRI and DECT scans from a subgroup of 10 patients were compared, using DECT as a gold standard, 2-reader MRI had a specificity of 0.98 [95% CI: 0.93 – 0.99], sensitivity of 0.63 [95% CI: 0.48 – 0.76], positive predictive value (PPV) of 94% and negative predictive value (NPV) of 84% for detecting tophi. There were only 2 instances in one patient where both MRI readers separately recorded tophus at a bone site where it was negative on DECT.
Conclusion: MRI has moderate to high reproducibility for assessment of gouty arthropathy and strong construct validity for detecting tophi when compared with DECT.
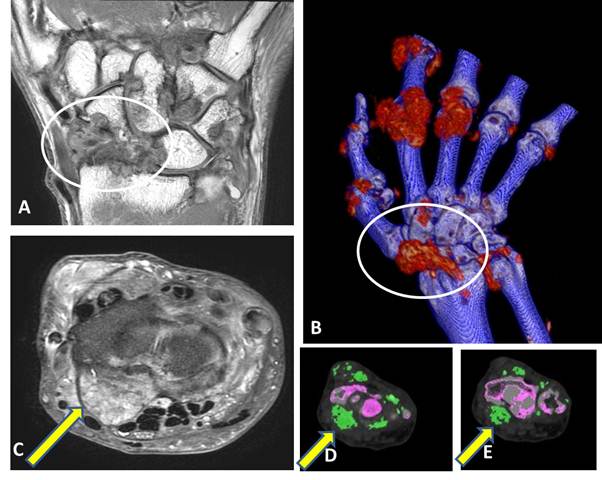
Figure: A) Coronal T1w MRI scan revealing extensive tophi dorsally at the radioscaphoid joint (circle). B) volume rendered DECT scan shows same tophus (circle) C) axial T1w MRI – tophus extends ventrally (arrow) D) axial DECT image shows same tophus (arrow) at level of the scaphoid and E) adjacent to the radius.
Disclosure:
F. M. McQueen,
None;
A. Doyle,
None;
Q. Reeves,
None;
A. Gao,
None;
A. Tsai,
None;
G. Gamble,
None;
B. Curteis,
None;
M. Williams,
None;
N. Dalbeth,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/magnetic-resonance-imaging-versus-dual-energy-computed-tomography-for-detection-of-joint-pathology-in-gout/