Session Information
Date: Sunday, November 8, 2015
Title: Osteoarthritis - Clinical Aspects Poster I: Treatments and Metabolic Risk Factors
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: The OMERACT
HOA working group recently proposed ‘hand mobility’ as an outcome measure in HOA
trials, although no disease specific instruments are available yet. We aimed to
investigate the construct validity of four hand mobility tests, validated in
other rheumatic diseases, in HOA and its subsets.
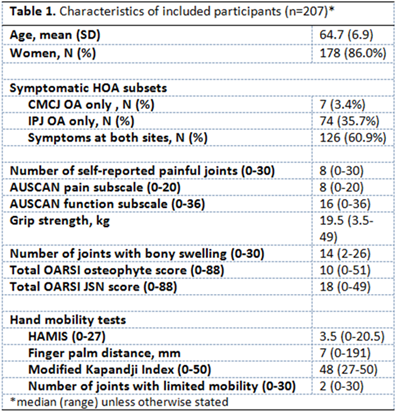
Methods: 207 participants from the Genetics ARthrosis and Progression study
with symptomatic HOA following ACR criteria completed standardized
questionnaires. Hand mobility was examined by trained assessors with the Hand
Mobility in Scleroderma test (HAMIS, scale 0-27, higher worse), fingertip to palm
distance (FPD, millimetres, higher worse), modified Kapandji index (MKI, 0-50,
higher better), and number of hand joints with limited mobility (0-30, higher
worse). Subscores for thumb base and finger HOA subsets were calculated for
HAMIS (thumb abduction and pincer grip (0-6), versus finger flexion, extension
and abduction (0-9)) and MKI (thumb opposition (0-10), versus finger flexion
and extension (0-40)). Radiographs were scored using OARSI atlas. With multivariable
linear regression the capability to measure unique concepts was investigated. Complete
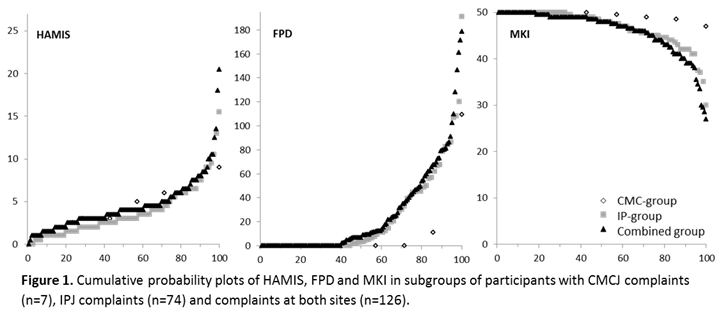
and (thumb/finger) subscores were compared in cumulative probability plots, exploring
whether scores differed between participants with complaints at different sites
(carpometacarpal joint (CMCJ) only, interphalangeal joint (IPJ) only and both
sites). Data were analysed in SPSS V20.0.
Results: Participants displayed large variation in mobility scores (table,
figure). Strongest correlations were with OARSI osteophyte score (rs
0.43-0.52), number of joints with bony swellings (rs 0.46-0.58) AUSCAN
function (rs 0.27-0.36), grip strength (rs 0.08-0.33) and
AUSCAN pain (rs 0.25-0.34). All tests showed similar correlations
with these outcomes, and in multivariable models 35-46% of the scores were
explained by a combination of structural damage, disability and strength; pain
and joint activity did not contribute substantially. Probability plots demonstrated
that FPD and MKI measure finger more than thumb mobility (figure). Additional
plots showed that subscores differ per HOA subset. Only HAMIS-derived thumb subscores
distinguished the CMC subset.
Conclusion: The tests show similar and acceptable levels of construct
validity. Despite a large variation in scores, they appear to measure in part a
unique domain. HAMIS, FPD and MKI perform similarly for finger mobility,
although only HAMIS can measure thumb mobility specifically. Other metric
properties and the potential of separate thumb- and finger-tests need to be
studied.
To cite this abstract in AMA style:
Kroon F, Bijsterbosch J, Meulenbelt I, Rosendaal FR, van der Heijde D, Kloppenburg M. Construct Validity of Four Hand Mobility Measures in Hand Osteoarthritis (HOA) [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/construct-validity-of-four-hand-mobility-measures-in-hand-osteoarthritis-hoa/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/construct-validity-of-four-hand-mobility-measures-in-hand-osteoarthritis-hoa/